

April 2013HOW OFCCP COVERS HOSPITALS |
I was going to write about the provocative way OFCCP currently selects contractors and contractor establishments for audit, but the tenor and volume of calls and e-mail traffic to my desk in the last two weeks from health care clients and industry representatives have persuaded me I need to wade NOW into the health care-OFCCP thicket. Apart from straightening out the welter of confusion regarding OFCCP's coverage of the health care industry, I discuss below how to value hospital contracts (which is very tricky, as it turns out). I also discuss what kinds of federal contracts are not covered and do not subject companies to OFCCP's jurisdiction if the companies receive these kinds of federal monies. And, along the way, I explain UPMC's four failed defenses to OFCCP jurisdiction over it and why all four lost arguments were entirely predictable (as I first predicted in 2006). There is also a lot of information in this posting about government contracting issues and strategies.
First, health care institutions were OFCCP's number one audit target in the most recent (March 27, 2013) round of OFCCP CSALs ("Corporate Scheduling Announcement Letters"…these are the so-called "Notice Letters" just giving a company a "heads-up" warning that OFCCP may soon be auditing them). Moreover, dozens of major hospitals are already receiving OFCCP audit Scheduling Letters setting the recipient hospitals down for immediate audit. (By the way, ignore all the OFCCP Blogs which have it absolutely wrong when they write that OFCCP is conducting "routine, random" audit selections. OFCCP got rid of "routine, random" selections of contractors for audit two years ago. OFCCP now targets industries…but that was the story I was going to write, with its numerous additional wrinkles and sub-topics, until OFCCP's health care audit barrage knocked that audit story to a later column. Ah, so little space, so much to write about with this active Administration.)
Second, how many major forms of federal contracts are there which can capture hospitals and medical clinics and subject them to OFCCP's jurisdiction as either a covered federal contractor or covered federal subcontractor? At least five: Let's together count the ways…
The Five Major Ways OFCCP's Jurisdictional Fishing Nets Capture Health Care Companies
- Federal Prison Contracts: The United States Department of Justice operates a sub department known as the Federal Bureau of Prisons ("BOP"). BOP has been closing many prison hospitals and clinics for several years now and is outsourcing three primary kinds of medical services and supply needs to private sector medical clinics and to acute care hospitals:
- Emergency room "walk-in" outpatient services (to replace the first aid clinics which many prisons used to operate within the prison walls); and/or
- Acute care services (the full range of medical services including especially: cancer treatments; cardiac services; hernias; pregnancy; etc. Is anyone surprised that federal prisoners are no more healthy than the general population?)
- Mental health counseling (psychiatric disorders; depression; organic brain syndrome, etc.)
NOTE 1 about contracting protocols: Most federal contracting officers, including BOP contract officers, usually write federal contracts for a one-year duration tracking the federal Fiscal Year (which runs October 1 through September 30). This is because most federal agencies get their budgets in one year increments.
NOTE 2 about contracting protocols: Most contracting officers, and we are seeing this with BOP contracting officers, write contracts with annual renewal authority making the contracts appear, at first blush, to be for either 3 or 5 years. Close examination of the contract, however, will reveal that the contract officers have usually written the typical one-year contract but have allowed for either 2 or 4 one-year extensions. So, each year, the contract is automatically extended for one more of the years authorized in the contract absent timely notice of termination by one of the parties (usually 90 or 30 days notice before the contract's annual termination date…usually on September 30). So, one values "the contract" not by the 3 or 5 year term, but rather by the value of each annual contract, since each one-year contract is a separate and distinct contract. NOTE: It is important to know how to value these contracts to determine not only whether OFCCP has proper jurisdiction over the contractor, but to also thereafter determine the type of compliance obligation the contractor has contractually committed to provide.
NOTE 3 about contracting protocols: Each one-year contract is typically a form of a master contract: what is known as an "open-ended supply contract" or what is sometimes called a "BPA" "Blanket Purchase Agreement"). Contract officers write these contracts when they are not making a one-time buy, but rather need medical services and/or supplies on a continuous but irregular and unpredictable basis. Accordingly, when the prison sends over patient # 1, that service request becomes a "call" upon the master contract in contract parlance. The "call" is not "the contract", but only one piece of the larger "open-ended supply contract". One values a BPA, or open-ended supply contract, NOT by the value of the "call", but rather by the value of all of the calls made during the Fiscal Year operation of the one-year contract. EXAMPLE: If the prison sent 3 prisoners over for treatment during the Fiscal Year and call #1 cost $5,000, call #2 cost $45,000 and call #3 cost $10,000, the value of that one-year contract would be $60,000. See OFCCP v. Star Machinery Co., 83-OFCCP-4, 1983 WL 411024 (Sept. 21, 1983–Secretary of Labor Raymond J. Donovan); 2 Empl. Prac. Guide (CCH) para 5102; 2 Aff. Action Compl. Man. (BNA) D:9101. [BPA valued by the value of all of the "calls" put against the BPA during the one-year operation of the BPA].
NOTE 4 about contracting protocols: Hospitals and clinics do not price their services and supplies like the grocery store with a set price one comes to expect plus or minus a little bit of change based on small daily tremors in the marketplace. Rather, hospitals and clinics have amazing flexibility and amplitude in pricing schedules. On the same day on the same floor of the same hospital, the same medical procedure can cost anywhere from X to 10X depending upon whether it is being billed to Medicare, to an insurance company, an HMO, or to an uninsured patient. (Just look at your hospital bill, or even the bill for your personal physician and note the reduced price from the "true cost" the insurance company pays the medical provider on your behalf.) So, in valuing contracts for the delivery of medical services and supplies, make sure you know what pricing schedule you are retrieving, or want to retrieve.
NOTE 5 about contracting protocols: Do not accept uncritically the face value reported on an open-ended supply contract (or BPA) since the amount shown is a maximum authorized "ceiling" amount. The reality may be far different. For example, OFCCP recently advised a small hospital chain I represent that it had a covered federal contract of $125,000 (which was in fact the face value of a covered federal contract the hospital had indeed signed). However, the federal agency which had signed the contract had in fact made only one call against the contract in the prior Fiscal Year (valued at only $2,000) and through the 5th month of the current Fiscal Year had drawn down no services, in fact. So, the contract value in FY 2012 was $2,000, and in FY 2013 the value was $0. PRACTICE TIP: always check either your records or the records of your client's federal agency contract officer (they know: they keep track).
- U.S. Veterans Administration Contracts: The VA is outsourcing the placement of protected veterans into private nursing homes (this is big business) and occasionally drawing down collateral medical services and supplies on behalf of veterans with rights to medical benefits and rehabilitation.
- Department of Defense Research Contracts: There seem to be two main types: robotics research contracts and mental health contracts (often studying Posttraumatic Stress Disorders: PTSD). While the United States Army is the world's leader in robotic rehabilitation, the Army is expanding its research and development of next generation limbs as a consequence of the large number of military personnel returning from the Middle East with arm and leg amputations and severe spinal cord injuries.
- Medical Supplies: Many agencies need to purchase medical supplies for their hospitals, medical care professionals and infirmaries. Many contract officers now not only buy medical supplies in the spot markets, but also do so over the phone and/or via the Internet using government issued credit cards. Senior contract officers increasingly have large charge allowances on their credit cards and may sometimes make a purchase in the spot market and over the phone for more than $50,000 (i.e. more than OFCCP's AAP-required threshold).
- U.S. Office of Personnel Management Contracts for Active Duty Civilian Employees: OPM has changed its architecture to supply medical services and supplies to its over 1-million active federal civilian employees. Rather than to purchase blanket Blue-Cross Blue-Shield coverage, as in the past, OPM is now contracting directly with hospital systems to cause them to provide medical services and supplies to federal civilian agency employees, both for emergency room services and for acute care treatment. These contracts can amount to many millions of dollars per year near federal enclaves. These are direct federal contracts and subcontracts to supply medical services and supplies…NOT to provide insurance.
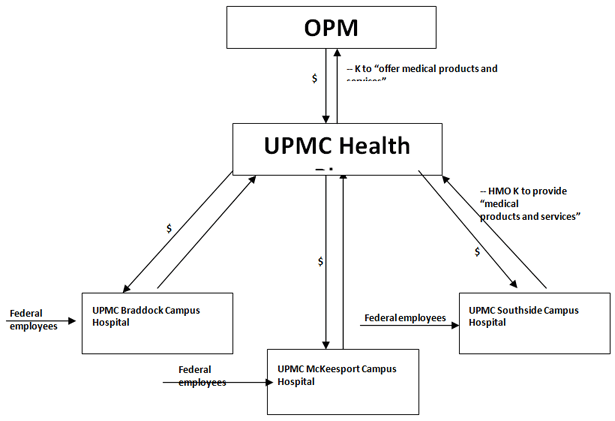
FACTS: In 2000, UPMC set up a Health Maintenance Organization (HMO) which in turn signed a contract with OPM to provide "medical services and supplies" for federal employees who chose to enroll in the Federal Employees Health Benefits Program OPM offered to its employees. (OFCCP contended this was a direct federal contract. It was). The HMOs, in turn, signed contracts with the three at-issue hospitals to provide "medical services and supplies" to the enrolled federal employees when those employees sought to exercise their HMO medical benefits. (OFCCP contended that these contracts running between the HMO and the three hospitals were federal "subcontracts" because the hospitals both subsumed the contract duties of the HMO and were "necessary to" the HMOs to satisfy their contract obligations to provide "medical services and supplies". The Court found these contracts to be federal "subcontracts"). See 4 CFR Section 60-1.3 (definition of "subcontract").
Here is what the OPM-UPMC contract facts look like, as I have reduced them to a graphic for easy inhalation:
 |
UPMC made these four failed arguments:
UPMC defense theory #1: The 3 hospitals are not covered because OPM expressly agreed in its contracts with the HMOs that providers of medical services and/or supplies would not be "subcontractors".
HELD: Private contracts cannot override the dictates of federal law. Look to OFCCP regulations to define who is a covered federal subcontractor.
UPMC defense theory #2: OFCCP's definition of the term "subcontractor" does not capture the hospitals since such contracts are for the "furnishing of property or non-personal services" (emphasis added) and the hospitals' contracts are for personal medical services to patients.
HELD: OFCCP's subcontract definition only allows OFCCP to cover "non-personal services". The question then becomes what is meant by "personal services" and is the UPMC contract to deliver "medical services" a "personal services" contract as UPMC argued. Answer: "No". In government contracts law, contracts for "personal services" are employment contracts. Accordingly, the UPMC contract is covered as a contract for "non-personal services" since the hospitals' contracts with the HMO were not contracts of employment. The "personal services exception" to OFCCP coverage thus avoids making the employees of federal contractors "subcontractors" by virtue of their employment contracts with the federal contractor.
UPMC defense theory #3: The OPM contract was a contract for insurance, via an HMO, and not for the delivery of "medical services and/or supplies" and thus the hospital contracts to deliver "medical supplies and services" were not "subcontracts" because the hospital contracts were not "necessary to" the HMO's performance of its contracts to deliver "insurance" to OPM.
HELD: HMOs provide both insurance and "medical services and supplies" as did the UPMC HMO. As a result, the UPMC hospital contracts were federal subcontracts because they both subsumed the contract obligations of the HMOs to OPM to deliver "medical supplies and services" and were "necessary to" the performance of the HMO's contracts to OPM to deliver "medical services and supplies".
UPMC defense theory #4: The hospital contracts did not contain OFCCP's 7 (EO)+13 (VEVRAA)+6 (Section 503) EEO Clauses. Thus, the hospitals never agreed to be bound by OFCCP's regulations.
HELD: "…the Government can compel [a company] to comply with the equal opportunity obligations of Executive Order 11246, even though the company has not expressly consented to be bound by that order." NOTE: OFCCP regulations vicariously insert the 7+13+6 EEO clauses into covered federal subcontractors as a matter of law. (i.e. you don't see them, but they are there nonetheless!).
So, UPMC v. Harris, in the end, turned out to be much ado about nothing (although it did buy 9 years of time for UPMC to get into compliance (OFCCP scheduled its audits of the three hospitals in January 2004).
Finally, unrelated to the UPMC case, what federal contracts are not "covered" and would not precipitate OFCCP jurisdiction over health care industry companies?
- Contracts to deliver "Federal Financial Assistance", colloquially known on the street as "grants". Grants do not provoke OFCCP jurisdiction. "Grants" are federal monies, but they are not "contracts". OFCCP's three program authorities (Executive Order 11246, Section 503 of the Rehabilitation Act and that portion of the Vietnam Era Veterans Readjustment Assistance Act which OFCCP enforces (known as 38 U.S.C. Section 4212)) all attach their compliance obligations (only) to federal "contracts" (and then only at varying levels of contract value: VEVRAA does not attach, for example, until a company signs "a" contract of $100,000 or more). NOTE: The Executive purports to also (uniquely) cover Federal Financial Assistance to construction contractors. Some prominent health care industry examples of (not OFCCP covered) "grants" include:
- Medicare is a "grant"…Thus, no OFCCP coverage attaches from a hospital or clinic's acceptance of Medicare payments. (OFCCP agrees)
- Medicaid is a "grant". (OFCCP agrees)
- Medicare Parts C&D (the new additions to Medicare) are "grants" as far as I can tell. No litigation on this yet. (Part C, called Medicare Advantage, allows Medicare beneficiaries to choose to receive all of their health care services through a provider organization). Part D is the new highly publicized prescription drug coverage option Medicare beneficiaries may elect and which costs are paid for by the monthly premiums of enrollees and by Medicare). OFCCP declines to speak to either issue. (OFCCP does not want to forfeit coverage, although I can find no principled legal argument for OFCCP to make that Part C and/or Part D are "contracts").
- Most FDA research contracts (often doled out to teaching or research hospitals) are "grants".
By the way: how does one know a "grant" from a "contract"? A "grant" is intended to serve a broad public purpose and to not service the parochial supply or service needs of the federal agency issuing the contract. Example: National Flood Insurance is a "grant" because it benefits the public generally and not the administrative survival needs of a federal agency. A DoD requisition for delivery of 5-gallon water bottles to military personnel training in the Mojave desert in summer is a federal contract designed to supply DoD with supplies and/or services the agency needs to function.
- Contracts to deliver Tri-Care medical services and supplies: The Congress in December 2011 exempted Tri-Care contracts from OFCCP coverage via Section 715 of the National Defense Authorization Act (the 2012 Defense Budget). The ARB subsequently upheld the exemption AND EVEN (SURPRISINGLY) gave it retroactive application to years prior to December 2011. (OFCCP v. Fla. Hosp. of Orlando, DOL ARB, No. 11-011, 10/19/12).
Tri-Care is a multi-billion dollar annual outsourcing of medical services from DoD to hospitals and clinics all over the United States to deliver medical services and/or supplies to (primarily) retirees of the armed services who have contract rights for life to medical benefits. As DoD has closed increasingly more and larger military reservations and bases, more and more military hospitals have closed forcing DoD to outsource to the private sector to fulfill its medical benefits contract guarantees to retired servicemen and women. (The Tri-Care exemption bill was one-of-a-kind legislation never previously seen and not likely to be seen again as to other forms of federal contracts in the future.) Of course, this special and unique legislation underscored just how much the health care industry feared OFCCP. OFCCP has now responded, in kind, by targeting hospitals and clinics for the "lion's share" of the remaining audits OFCCP will schedule in calendar 2013. (There is a saying in the very small Silicon Valley which seems apropos: "What goes around comes around"). - Prime federal contracts to deliver "medical insurance" do not render resulting medical service and supply contracts "necessary to" the performance of the prime insurance contract. That is the Bridgeport Hospital case on which UPMC so desperately, and unsuccessfully, tried to model its defense. See, OFCCP v, Bridgeport Hospital, ARB No. 00-034, ALJ No. 1997-OFC-1 (ARB Jan. 31, 2003).
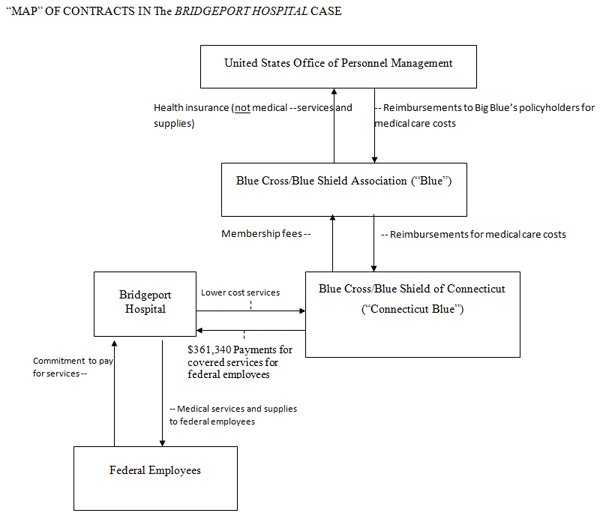
In the Bridgeport Hospital case decision, the Administrative Review Board (the administrative appeals court of last resort within the U.S. Department of Labor) held that the Bridgeport Hospital was NOT a "federal subcontractor" when OPM purchased "medical insurance" for its civilian employees through Blue Cross/Blue Shield of America (making it a direct federal contractor: not a dispute in the case). BC/BS contracted, in turn, with BC/BS of Connecticut to similarly provide "medical insurance" to civilian employees in Connecticut (making it a federal subcontractor: not a dispute in the case). BC/BS of Connecticut, in turn, signed a contract with the Bridgeport Hospital in Bridgeport, Connecticut to provide "medical services and medical supplies" to federal employees who sought medical services from the Hospital and presented their BC/BS card. When OFCCP subsequently tried to audit the Bridgeport Hospital, the Hospital protested and explained it was not a "subcontractor" because its provision of "medical services and medical supplies" was not "necessary to" BC/BS Connecticut to perform its contract to supply "medical insurance". Said another way, medical services and supplies did not equal medical insurance. The Administrative Law Judge and thereafter, the ARB, agreed, and OFCCP lost.
Here is a graphic depicting the facts of the Bridgeport Hospital case:
Three final notes:
(1) Hospitals are large and complex (from a legal point of view) employers of employees. They are attractive targets for OFCCP auditors. There are many job classifications and employment systems of great interest to OFCCP auditors, and because of their size and complexity, and lack of prior OFCCP "conditioning" to audits, DO NOT UNDERESTIMATE THE TIME TO CONVERT HEALTH CARE COMPANIES TO OFCCP-COMPLIANT STATUS. I use the normal rule of Law Firm Partner time estimation of work they assign to junior associates: multiply by two and add one and you will be close to the reality of the time actually needed to do the work called for: in this case, convert a "virgin employer" to an OFCCP-compliant federal contractor. You will find many data systems missing, in my experience, and many non-standard and informal employment practices and systems.
(2) Many health care companies have potentially problematic employment law issues of great interest to OFCCP. Proceed with caution and put the entire conversion to federal contractor status under attorney-client privilege.
(3) Look VERY hard first at the contract coverage issues to make sure your hospital is indeed OFCCP covered. And think very hard and long about whether your hospital wants to be, or to remain, a federal contractor. That is a policy and economic choice. But my advice for several decades has been and remains to any wannabee federal contractor or any low-dollar-value federal contractor: "The Executive Order Compliance obligations do not scale. If you are going to "get into the water", don't just poke your toes in: Get in up to your neck". You need to capitalize the costs of your OFCCP compliance systems. Doing a poor job because of the numerous hidden compliance costs, often costs more in the long run than properly complying. If the value of the federal contract(s) the Hospital has do not at least equal the cost of compliance, consider ceasing to be a federal contractor. How to terminate federal contracts, though, is another lengthy and complex discussion (although entirely doable)…just don't crawl out of the water, once in, without a lifeguard present. It can be a tricky exit under government contracting regulations.
Thanks…John
| THIS COLUMN IS MEANT TO ASSIST IN A GENERAL UNDERSTANDING OF THE CURRENT LAW AND PRACTICE RELATING TO OFCCP. IT IS NOT TO BE REGARDED AS LEGAL ADVICE. COMPANIES OR INDIVIDUALS WITH PARTICULAR QUESTIONS SHOULD SEEK ADVICE OF COUNSEL. |